Best Post Cycle Therapy (PCT): Dr. Scally’s Protocol
 Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
Post-cycle therapy (PCT) is the phase when a bodybuilder utilizes medication(s) to restore endogenous (natural) testosterone production.
Anabolic steroids impair the hypothalamic-pituitary-testicular axis (HPTA) function, as the body detects excessively high serum testosterone levels.
Consequently, the body signals to cease testosterone production in a bid to maintain homeostasis by inhibiting gonadotropin-releasing hormone (GnRH).
This decreases the release of luteinizing hormone (LH) and follicle-stimulating hormone (FSH), two hormones crucial for testosterone synthesis.
Thus, when a bodybuilder comes off steroids and exogenous testosterone is removed, natural testosterone often shuts down.
This can result in various psychological and physiological side effects. The most common are:
- Decreased well-being
- Low libido
- Erectile dysfunction
- Catabolism (muscle loss)
- Decreased sperm count
- Testicular atrophy
The severity of the above effects depends on the anabolic steroids used, the dosages, and the length of the cycle.
We find that low testosterone can persist for several weeks or months post-cycle, increasing the likelihood of addiction due to strong withdrawal symptoms lingering.
The aim of a PCT is to dramatically shorten this process, thus accelerating the recovery of natural testosterone production. Bodybuilders at our clinic have reported taking the following substances to restore the HPTA:
- Clomid (clomiphene)
- Nolvadex (tamoxifen)
- Human chorionic gonadotropin (hCG)
The best PCT protocol
Dr. Michael Scally is one of the leading medical experts in hormone therapy, having specialist knowledge in regard to anabolic steroid-induced hypogonadism (ASIH).
After treating hundreds of patients, Dr. Scally developed a PCT protocol that was used in a clinical report to treat 19 healthy men. All of these men had extremely suppressed testosterone levels as a result of using testosterone and Deca Durabolin for 12 weeks.
The following protocol successfully treated 100% of the male subjects, bringing their serum testosterone levels back to normal levels (within 45 days). This is quite a feat, considering it is common for bodybuilders to experience low testosterone for up to 4 months following a steroid cycle.
- HCG: 2000 IU is administered every other day for 20 days.
- Tamoxifen (Nolvadex): 2 x 20 mg for 45 days
- Clomiphene (Clomid): 2 x 50 mg for 30 days
The above post-cycle therapy plan should be viewed as aggressive. Consequently, if potent AAS are used, our bodybuilding patients have reported the protocol to be highly effective.
However, if milder steroids are used (such as Anavar, Primobolan, or Turinabol), testosterone levels may only be moderately suppressed (rather than completely shut down). In this case, all three of these PCT medications taken simultaneously may not be necessary.
The timing of a PCT is crucial regarding its effectiveness. If it begins too early, we often find it ineffective because exogenous testosterone is still present in the body. If started too late, the body will have already entered a catabolic state, with withdrawal symptoms already occurring.
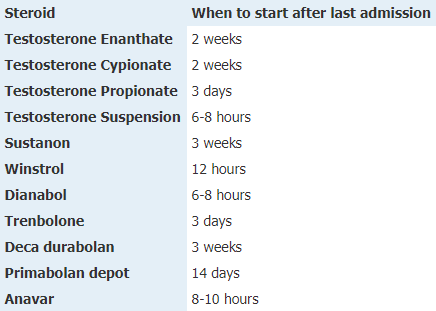
The timing of a PCT should be tailored to the half-life of the steroid(s) taken. If users are taking multiple AAS simultaneously, then a PCT should begin after the last compound clears out of the body, i.e., the slowest.
Here is a guide so users know when to start their PCT:
Clomid
Clomid is a selective estrogen receptor modulator (SERM), often prescribed to women as a fertility drug, acting as an ovulatory stimulant.
Clomid increases the secretion of gonadotropins (LH and FSH) via the inhibition of estrogen in various tissues, leading to an increase in endogenous testosterone.
Despite blocking estrogenic effects in many parts of the body, Clomid increases estrogen activity in the liver, causing a positive shift in cholesterol levels. This is particularly useful in regulating blood lipids and easing cardiovascular strain in our patients post-cycle.
Clomid side effects
Our patients have reported visual changes occurring on Clomid when they have taken it in high doses.
This includes flashes or blurring; however, these are often temporary in our experience and subside within a few days or weeks post-cycle.
It is unknown what causes such alterations in vision. In very rare cases, such side effects have the potential to be irreversible, but we have yet to see this happen.
If ocular changes start to occur, users should discontinue Clomid supplementation immediately and visit an ophthalmologist for an urgent examination.
More common side effects of Clomid, in our experience, include:
- Flushes
- Abdominal discomfort
- Nausea
- Headaches
- Liver stress
- Impaired eyesight
Nolvadex

Nolvadex (tamoxifen citrate) is a SERM commonly prescribed to women with breast cancer and is regarded as one of the main reasons why the mortality rate for breast cancer sufferers has significantly dropped in the last decade.
Nolvadex was first synthesized in 1962 and initially prescribed to treat female infertility.
However, it was later observed to have anti-mitogenic effects, reducing the stimulation of breast tissue and being beneficial for slowing the growth of breast cancer.
Nolvadex also exhibited cancer-killing properties due to the blocking of protein kinase C (PKC) via oxidative stress mechanisms (1).
Bodybuilders who see us commonly use Nolvadex to prevent the onset of gynecomastia (the accumulation of breast tissue).
As a PCT, Nolvadex works in the same way as Clomid, stimulating LH and FSH production via the inhibition of estrogen’s negative effects in the hypothalamus (and thus restoring the HPTA).
Nolvadex side effects
- Skin rash
- Hot flashes
- Decreased white blood cell count
- Visual disturbances
- Blood clots (deep vein thrombosis)
- Liver stress
Uterine sarcoma and endometrial cancer have been linked to Nolvadex use. However, the American Cancer Society states that the risk is very low, at approximately 1 in 500 cases. Such side effects are also correlated with long-term use (more than 2 years). This is not something we have seen in our clinic as of yet.
HCG
HCG (human chorionic gonadotropin) is a hormone produced by women in high quantities in the early stages of pregnancy, facilitating an increase in progesterone and helping to nurture the developing fetus and its surrounding environment (preventing miscarriage).
HCG taken post-cycle can elevate LH levels, stimulating the Leydig cells to produce more endogenous testosterone.
- HCG has not only been used in the treatment of male hypogonadism but also for obesity.
- It was previously believed that hCG may have a stimulating effect on T3 levels; however, we have not observed this.
- However, we have found hCG to have appetite-suppressant effects, meaning people can eat very low-calorie diets without feeling excessive hunger.
In 1957, hCG became the most prescribed medication for weight loss due to its powerful (yet indirect) effect on satiety.
We have found hCG to be the most effective post-cycle therapy medication for treating testicular atrophy (shrinkage) due to its spermatogenesis-inducing effects.
HCG side effects
The most common adverse effects of hCG are bloating and pain in the pelvic region.
Rarer side effects include:
- Nausea
- Diarrhea
- Indigestion
- Acne
- Lack of appetite
- Tiredness
- Headaches
- Shortness of breath
PCT for women
PCT is often deemed unnecessary for women, which may stem from their smaller quantities of endogenous testosterone.
As with men, women’s endogenous testosterone production will also shut down due to the body detecting an excess of this male hormone.
In our experience, testosterone remains a crucial hormone in females, greatly affecting their:
- Libido
- Well-being
- Energy
- Muscle mass
We see that when testosterone declines, estrogen also drops significantly due to less aromatization (conversion of testosterone into estrogen).
Dave Crossland states that he has anecdotal evidence of female steroid users experiencing very low estrogen levels, low mood, diminished libido, and depression post-cycle.
HCG is not an optimal PCT medication for women, as it can cause virilization and enlargement of the ovaries. Clomid may also not be optimal due to ovarian hypersensitivity.
An off-label medication commonly used by female bodybuilders deficient in androgens is dehydroepiandrosterone (DHEA). DHEA is one of the most critical hormones in females, being a key precursor of androgen and estrogen synthesis (2).
One study found that 50 mg/day of DHEA significantly increased libido in women over 70 years old when taken for 1 year (3).
Another study found that a 6-week cycle of DHEA improved sexual function in women, including arousal, orgasm quality, and libido (4). They also found that depression symptoms decreased by 50%, significantly improving mood.
These women took 90 mg/day of DHEA for the first 3 weeks, followed by 450 mg/day of DHEA for the remaining 3 weeks.
Other research (Morales et al. 1994) has shown that 50 mg/day of DHEA, when administered for 3 months, improves well-being in women by 82% (5). They also reported:
- Greater relaxation
- Improved sleep
- Less stress
- Higher energy levels
Our female patients have reported 50 mg/day of DHEA for 12 weeks being effective as a PCT. However, DHEA is not FDA-approved for restoring endogenous testosterone levels in women, and therefore, we do not endorse its use.
Frequently asked questions
Is a PCT essential?
Post-cycle therapy may not be considered essential, as natural testosterone levels typically recover in most steroid users. However, a better question may be, is a PCT optimal?
The answer to this is yes, as not only will users retain more of their gains from a cycle, but they will also improve their mental and sexual health.
We have found that a PCT can be less essential when taking mild AAS, such as Anavar, with our tests showing a moderate reduction of 45% when taking 20–40 mg/day of Anavar for 12 weeks (6).
How do I know if I need a PCT?
The most accurate way to know if you need a PCT is to get your testosterone levels checked.
However, if you have reasons for not wanting to see a doctor, you can often tell from the following signs:
- Depression
- Low libido
- Testicular atrophy (shrinkage)
- Muscle atrophy
Where do bodybuilders buy PCT supplements?
Bodybuilders often purchase PCT supplements on the black market (in the same way they buy anabolic steroids). However, this method involves asking around and finding a source where you can pay with cash or by making a payment online (which is risky if you enter your card details).
How much do PCT supplements cost?
A reliable supplier of anabolic steroids has provided us with the US prices of drugs used by bodybuilders for PCT:
- Clomid 50 x 50 mg tablets: $49
- Tamoxifen (Nolvadex), 50 x 20 mg tablets: $49
- HCG 11,000 IU: $75
Do SARMs require a PCT?
SARMs can be suppressive according to existing research, so a PCT can be deemed necessary. However, we assess the severity of the decline in testosterone before determining the PCT protocol and how aggressive it should be.
As with steroids, we see certain SARMs causing greater declines in endogenous testosterone than others.
However, as a general rule, if users take one SARM, they should stick to a low to moderate dosage and cycle it for 8 weeks or less; only a moderate decline in testosterone is likely to occur.
In this case, bodybuilders may supplement with Nolvadex for 3 weeks to bring endogenous testosterone levels back to normal, with 30 mg/day taken for week 1, 20 mg/day for week 2, and 10 mg/day for week 3.
If slightly higher dosages are taken or longer cycles are utilized, Nolvadex is commonly taken for 4 weeks, starting at 40 mg for week 1, then decreasing the dosage by 10 mg each week for the remaining 3 weeks.
For a high-dose SARM cycle, a 4-week Nolvadex PCT is more frequently employed, being 40 mg/day during weeks 1 and 2, then 20 mg/day during weeks 3 and 4.
We have seen some individuals take risks with SARMs, i.e., stacking several compounds together, such as combining Ostarine, RAD-140, and LGD-4033 in excessively long cycles lasting 12–16 weeks. In this case, we find that a more drastic PCT protocol is needed.
Note: Some people mistake certain compounds for SARMs, such as Cardarine and MK-677. These are not SARMs and thus do not require a PCT, with Cardarine being a peroxisome proliferator activator receptor delta (PPAR-delta) and MK-677 being a growth hormone secretagogue.
How much muscle will a PCT help keep?
We have seen effective PCTs help retain up to 80% of lean muscle gains from a cycle.
Mild compounds, such as Anavar or Primobolan, may enable users to retain high amounts of muscle tissue. This is because of less dramatic peaks in exogenous testosterone levels on-cycle (and thus less endogenous shutdown).
Note: It is normal to lose some weight when coming off steroids, particularly when utilizing wet, bulking compounds, with users losing some intracellular and extracellular fluid that previously accumulated due to high estrogen levels. This should not be confused with losing muscle weight.
What are the least suppressive anabolic steroids?
We have observed Anavar and Primobolan to exhibit the lowest degree of suppressive effects among anabolic steroids. Additionally, it should be noted that these substances present modest hepatotoxic and cardiotoxic properties, rendering them one of the most secure anabolic-androgenic steroids (AAS) available on the market.
PCT diet and supplementation
In our experience, a person’s diet can also help to increase testosterone and anabolism post-cycle.
Our consultant, Dr. George Touliatos, has found eating a diet rich in meat and egg yolks to be an effective protocol, with cholesterol being a steroid hormone that synthesizes testosterone.
Research has also found a link between higher HDL levels and high testosterone in males (7).
Dr. Touliatos also states that ZMA, d-aspartic acid, tribulus terrestris, maca, and vitamin D3 supplements can help maximize natural testosterone production.
PCT pros and cons
Pros:
- Increases testosterone production (8, 9)
- Improves well-being
- Enhances energy
- Helps to retain lean muscle
- Increases testicular size
- Increases libido and erection quality
- Improves fertility (10)
- Affordable
Cons:
- More expense (on top of steroids)
- Some compounds come with side effects (for sensitive users)
Co Authors :

Dr. Thomas O’Connor is the first American board-certified internist to focus his medical practice specifically on the health and recovery of individuals who use anabolic steroids and androgens.
He founded Testosteronology®, a dedicated subspecialty of internal medicine that addresses steroid-induced hypogonadism and associated cardiovascular and metabolic concerns.
Dr. O’Connor has over 20 years of experience treating men and women with a history of anabolic steroid, SARM, and PED use. He has been a board-certified MD since 2005 and provides guidance on harm reduction methodologies.
Dr. O’Connor is a clinical instructor at the University of Connecticut School of Medicine and has been featured in various media publications, including Generation Iron, Dr. Phil, National Geographic, The New York Times, Muscle and Fitness, and others.
Dr. O’Connor also co-authored the largest survey on anabolic steroid use, which involved 2,385 men and was published in the peer-reviewed American Journal of Men’s Health. He holds active medical licenses in Connecticut and Florida.
References
(1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4756695/
(2) https://academic.oup.com/humupd/article/13/3/239/2457836
(3) https://pubmed.ncbi.nlm.nih.gov/10760294/
(4) https://pubmed.ncbi.nlm.nih.gov/15699292/
(5) https://www.researchgate.net/publication/15684493_Effects_of_replacement_dose_DHEA_in_men_and_women_of_advancing_age
(6) https://pubmed.ncbi.nlm.nih.gov/16540931/
(7) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2666971/
(8) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5508437/
(9) https://pubmed.ncbi.nlm.nih.gov/22951175/
(10) https://www.ncbi.nlm.nih.gov/books/NBK559292/#:~:text=Clomiphene%20citrate%20is%20commonly%20indicated,male%20infertility%20to%20induce%20spermatogenesis.
