23 Questions & Answers About Steroids
 Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
An array of questions often surrounds the topic of anabolic steroids, with people either thinking about taking them or curious about their effects.
Asking questions can be a great method of learning; however, there remains a scarce amount of information online due to the taboo nature of steroids, causing much misinformation and bro-science.
Sadly, this may lead to vulnerable people causing themselves harm due to a lack of expert content being published.
Thus, in this guide, we will answer the most common questions regarding anabolic steroids (strictly for harm reduction purposes). Consequently, our readers can understand how they truly affect over 3 million people in America today, based on existing medical research and our own anecdotal findings.
Contents
- 1 Are steroids bad for you?
- 2 Are steroids illegal?
- 3 Did Arnold Schwarzenegger take steroids?
- 4 How much do steroids cost?
- 5 How much muscle will I gain on steroids?
- 6 Are the effects of steroids permanent?
- 7 Will I get acne?
- 8 Will steroids affect my sex drive?
- 9 Do I need to run a PCT?
- 10 Can anabolic steroids make you depressed?
- 11 Where do I inject steroids?
- 12 Do steroids make your penis smaller?
- 13 How to prevent gynecomastia?
- 14 Which steroids don’t cause gynecomastia?
- 15 Can steroids cause erectile dysfunction?
- 16 Are orals worse than injectables?
- 17 Can anabolic steroids be used in a non-toxic way?
- 18 How fast do steroids work?
- 19 Do steroids make you angry?
- 20 Do steroids show up on a drug test?
- 21 Do steroids cause hair loss?
- 22 Can steroids make you infertile?
Are steroids bad for you?
Yes, anabolic steroids are bad for you in the sense that cardiovascular side effects are certain, at least to some degree, no matter what compound you are taking.
This is due to all steroids being forms of exogenous testosterone and thus having a negative effect on high-density lipoprotein (HDL) and low-density lipoprotein (LDL) cholesterol.
We have found other side effects (unrelated to the heart) to be common, including:
- Liver damage
- Acne vulgaris
- Benign prostatic hyperplasia (prostate enlargement)
- Hypogonadism (low testosterone)
- Androgenetic alopecia (hair loss)
- Water retention
- Gynecomastia
There are steroids that cause mild effects, are well tolerated, and are even approved by the FDA (such as Anavar, Deca Durabolin, and testosterone).
There are also harsh steroids that have a detrimental effect on various organs and can even lead to death.
Therefore, a better question could be, “Are steroids worth the risk?”
In which case, this will depend on a person’s individual goals and what they are willing to risk.
If someone with a history of heart disease in their family is thinking of taking toxic steroids such as Dianabol or Anadrol on a regular basis, this is most likely a bad idea.
However, we have had patients who understand the risks and are happy to put their health (or life) at risk in order to win a bodybuilding trophy. In this instance, steroids are worth it to them (at least in the short term).
Are steroids illegal?
Yes, anabolic steroids are illegal to use for cosmetic purposes in almost every country in the world, with a couple of exceptions, such as Mexico and Thailand.
In America, they are classified as Schedule III controlled substances, and in the UK, they are Class C drugs.
However, steroids are legal to use when a person has been prescribed them for medicinal purposes.
For example, we can prescribe a man suffering from hypogonadism testosterone cypionate for TRT (testosterone replacement therapy) to bring his levels back into a normal range.
Anabolic steroids used to be legal for recreational purposes, with bodybuilders from the Golden Era simply making an appointment with their doctor (if they wanted to take Dianabol) to build more muscle.
However, little was known regarding the side effects in these initial stages, and thus they were not banned by the FDA.
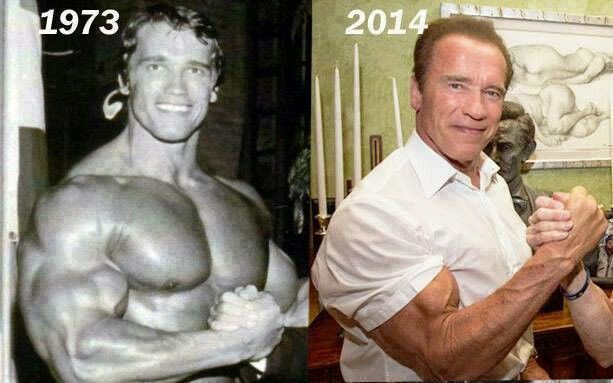
Did Arnold Schwarzenegger take steroids?

Yes, Arnold Schwarzenegger has admitted to taking steroids, mentioning that 60 years ago, bodybuilders were naïve to the long-term effects of these drugs.
Bodybuilders in Arnold’s era have hinted at certain compounds used, namely, Dianabol, Primobolan, and Deca Durabolin.
In Arnold’s book, Total Recall, he said he had heard about the East Germans and Soviets taking AAS to increase their performance. Upon hearing this, he would then visit his doctor to try them himself.
Arnold also mentioned there weren’t any rules surrounding steroids, so they weren’t banned or considered taboo like in sports today.
Based on the PEDs used in this era, we have a very good idea about the specific steroids given to Arnold during his first cycle.
In the context of this passage in Arnold’s book, his main objective was to build significantly more muscle and to look huge on stage, blowing away the crowd and judges.
Therefore, we know that these were mass-building agents, with one being an injectable and another an oral.
We also know the injectable was administered every 2 weeks, with at least one compound producing water retention (as Arnold mentions in the next passage that his gains were mostly water weight).
Dianabol (methandrostenolone) perfectly describes the oral pill that Arnold was prescribed.
The injectable steroid was thought to be Primobolan, a popular injectable in the ’60s and ’70s. This is practically confirmed in Frank Zane’s training diary, ‘Mind, Body, Spirit’ (see below):
“Diana bowl” refers to Dianabol, and “Prima bowl” to Primobolan.
We also know the dosages used in this cryptic poem, with ‘100 miles’ representing 100 mg of Primobolan per week. And 15 “milly gramola” represents 15 mg of Dianabol per day.
How much do steroids cost?
We have obtained the following price list from an (anonymous) trusted source within the bodybuilding community.
These are UK prices; however, we have added the US dollar equivalent in brackets (correct conversion at the time of publishing).
Cost of injectable steroids
- Testosterone Enanthate 250 mg/ml (25 amps): £120 / $167
- Testosterone Propionate 100 mg/ml 10 ml vial (25 amps): £45 / $63
Thus, a testosterone enanthate cycle, dosed at 300 mg for 8 weeks, would cost roughly £50 / $69.
Cost of oral steroids
- Anavar 100 x 20 mg tablets: £165 / $229
- Dianabol 1000 x 5 mg: £190 / $264
- Winstrol 100 x 25 mg tablets: £65 / $90
Cost of PCT drugs
- Clomid 50 (50 mg) tablets: £35 or $49
- Tamoxifen (Nolvadex) 50 (20 mg) tablets: £35 or $49
Cost of fat loss drugs
- Clenbuterol 400 (20 mcg) tablets: £70 or $97
- Ephedrine 100 (30 mg) tablets: £25 or $35
Readers should be cautious of sellers offering prices at a fraction of these, as the product is likely to be diluted or a placebo.
How much muscle will I gain on steroids?
The amount of muscle a person will gain on steroids will depend on the compounds used, their genetics, training, and nutrition.
Anavar is moderately anabolic, so it may only result in 15 pounds of muscle gain in our experience.
However, we have found trenbolone to produce 30 pounds of lean muscle tissue in a single cycle.
Bulking agents are the type of steroids that will produce the most muscle and weight gain, as opposed to cutting agents.
Here is a list of bulking steroids:
- Anadrol
- Dianabol
- Testosterone
- Deca Durabolin
- Trenbolone
- Superdrol
In the long term, we have seen men gain 50–60 pounds when transitioning from natural to steroids after administering several cycles.
Are the effects of steroids permanent?
There is clinical evidence to suggest that steroids do have a permanent effect on myonuclei inside the muscle cells (1).
In one study, a group of untrained mice was administered steroids (testosterone), causing exceptional muscle growth.
Then, when the steroid cycle ended, they returned to their original size.
However, when these mice later performed weight training (without any steroids), they grew 30% more compared to the group that had never used anabolics.
This indicates that muscle gains will be lost from taking steroids if a person becomes sedentary. We have also observed this to be true.
However, steroid gains may be maintained later on (naturally) if users continue lifting weights.
Arnold Schwarzenegger may be a perfect example of this permanent effect, displaying exceptional muscularity when training in old age.
There is also evidence to suggest that steroids’ adverse effects on visceral fat (VF) are permanent.
One study found that men who had previously taken steroids had higher levels of VF compared to non-steroid users (2). This is fat that surrounds the organs and cannot be seen by the naked eye, but high levels can push the abdomen out, creating a ‘protruding’ appearance. This is also known as steroid gut in the bodybuilding community and is initially caused by impaired insulin sensitivity.
Thus, even if someone stops using steroids, they will maintain a higher visceral body fat percentage later in life.
Will I get acne?

Acne vulgaris is a common androgenic side effect that we see in our clinic. Some compounds are worse at aggravating acne in users, with acne-prone individuals usually deciding to avoid such compounds. They may also opt for a compound with a reduced 5α-reductase conversion.
Treatment with antibacterial creams containing benzoyl peroxide has been effective for many of our patients in reducing acne through the removal of dead skin cells. If acne persists, then the employment of an antibiotic course can be successful.
Some may opt to source Accutane, a drug that has potent effects in reducing activity in the sebaceous glands. Such glands are responsible for producing excess amounts of an oily substance known as sebum. Accutane thus helps in treating the root cause of acne (excess sebum production blocking the pores).
Accutane (also known as Roaccutane by manufacturers ‘Roche’) is a very potent drug; however, its use should not be taken lightly. We have seen it cause various side effects, including mental health issues and suicide. However, in our experience, many users typically only notice mild effects such as drying of the nose, skin, ears, eyes, and joints.
Accutane is often difficult to obtain on the black market, and its high market price reflects this.
Will steroids affect my sex drive?
Yes, we often see strong androgens increasing libido in many users.
We also find weak androgen compounds (such as Deca Durabolin) having the opposite effect.
In this case, stacking Deca Durabolin with an androgenic compound (such as testosterone, Anadrol, or trenbolone) can help mitigate any decrease in sexual interest.
Note: After a steroid cycle ceases, sex drive may decrease due to decreased endogenous testosterone. These symptoms may persist for several weeks or months, depending on the compounds used and the PCT (post-cycle therapy) protocol.
Do I need to run a PCT?
Steroid users do not necessarily need to run a PCT, especially if mild compounds are utilized, such as Primobolan and Anavar. Such steroids only have a moderately lowering effect on endogenous testosterone levels, based on our SHBG tests.
Yet, in many cases, a PCT will help users recover physiologically and psychologically after a cycle.
No bodybuilder wants to experience low testosterone for several months after a cycle; thus, an effective PCT can significantly reduce this waiting period.
From a physical perspective, we find that a PCT keeps the body in an anabolic (muscle-building) state, cementing results from a cycle. Also, our patients report improved sexual health, which can often deteriorate post-cycle, causing less libido and weaker erections.
Men can often report feeling fatigued and having low energy post-cycle, which is a common side effect of low testosterone.
Psychologically, a PCT can help a man feel more confident and experience greater well-being due to testosterone increasing dopamine levels in the brain. Dopamine is a neurotransmitter that makes a person feel good; however, when low, it can contribute to depression or anxiety.
Can anabolic steroids make you depressed?
Yes, we have seen anabolic steroids cause depression in certain individuals due to the lowering of endogenous testosterone. As explained in the above section, testosterone increases dopamine, an important neurotransmitter for mental health. After a cycle ends, a man’s testosterone levels become shut down, and thus his mental health can suffer (at least temporarily).
Are steroids addictive?
We have found anabolic steroids to be very addictive for many individuals due to their remarkable effects on body composition and mental well-being.
Research suggests that roughly 1 million Americans have experienced a dependence on anabolic-androgenic steroids (3).
Such dependency may cause users to regret taking steroids later in life, with Sergio Oliva (one of the greatest bodybuilders of all time) reportedly stating that steroids were a “monkey on his back.”
Typically, patients under our care are only eager to come off steroids if they are experiencing serious health problems.
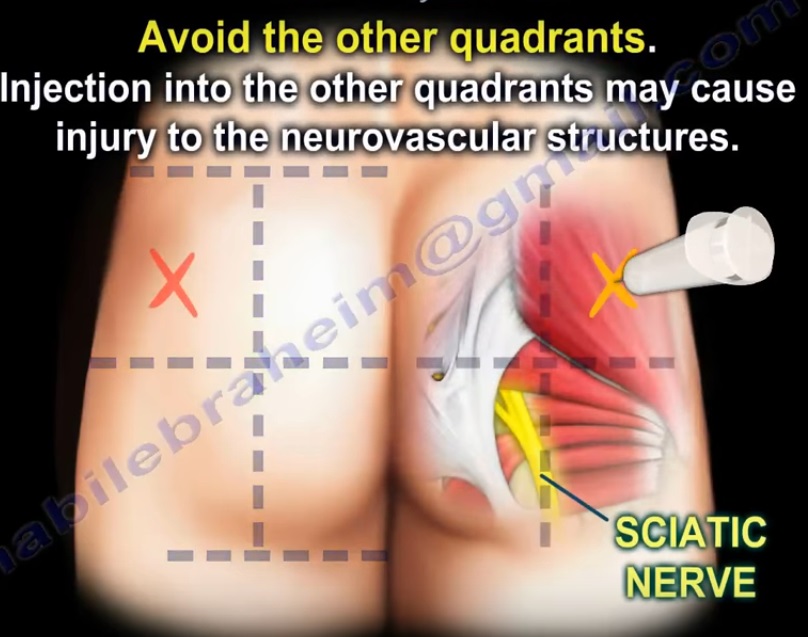
Where do I inject steroids?
The gluteus maximus, otherwise known as the backside, is a common choice for injections due to it being a large and deep muscle.
This is a favorable injection site for beginner steroid users due to the fact that it requires less precision.
It is important to inject intramuscularly, i.e., into the muscle.
Bodybuilders should avoid injecting into the vein, as this can result in serious implications, such as paralysis or death.
Do steroids make your penis smaller?
No, contrary to bodybuilding mythology, anabolic steroids have never caused penis shrinkage in any of our patients.
Equally, anabolic steroids do not cause any notable increase in penis size.
However, steroids do cause testicular atrophy (testicular shrinkage) due to them shutting down endogenous testosterone levels. We find this effect to be temporary, and thus, when testosterone levels return to normal (post-cycle), the testes are restored to their previous size.
How to prevent gynecomastia?
Gynecomastia is caused by excess estrogen levels. This female sex hormone can rise to exceptionally high levels on steroids due to high levels of aromatization (converting testosterone into estrogen).
In a bid to prevent gynecomastia, we find AIs (aromatase inhibitors) and SERMs (selective estrogen receptor modulators) to be effective.
AIs work by blocking the conversion of testosterone into estrogen, whereas SERMs do not stop this conversion but instead directly inhibit estrogen’s effects in the mammary glands.
We prefer to utilize SERMs, as we commonly find AIs worsening hypertension. This is because high estrogen levels have a positive impact on HDL cholesterol.
Which steroids don’t cause gynecomastia?
In our experience, any steroid that doesn’t provoke surges in female hormones, including estrogen or progesterone, is very unlikely to cause gynecomastia.
Some of the safer compounds for gyno are:
- Anavar (Oxandrolone)
- Winstrol (Stanozolol)
- Turinabol (Chlorodehydromethyltestosterone)
- Superdrol (Methasterone)
Anadrol, Dianabol, and testosterone are particularly estrogenic steroids and are thus likely to cause breast tissue expansion in sensitive individuals.
Can steroids cause erectile dysfunction?
Although steroids are likely to improve erection quality, yes, it is possible to experience erectile dysfunction (ED) with some compounds. Deca Durabolin is notorious for causing ED when used by itself, due to its reduced androgenicity.
We see weak androgenic steroids like Deca Durabolin reduce nitric oxide production, which is responsible for optimal blood flow to the penis. However, we found that stacking testosterone with Deca Durabolin for additional androgenicity maintains optimal circulation to the penis.
Are orals worse than injectables?

Many oral steroids are hepatotoxic, thus making them worse than injectable steroids from a hepatic health perspective.
Also, oral steroids can present more issues in relation to cardiovascular health due to their negative impact on hepatic lipase when being processed by the liver. This often causes greater fluctuations in cholesterol, increasing the risk of cardiac hypertrophy and heart disease.
However, there are a few oral steroids that do not pose serious risks to the liver and heart and have been well tolerated by many of our patients. Anavar, Primobolan (methenolone acetate), and testosterone undecanoate are examples of such compounds.
Equally, some injectable steroids can have detrimental effects on the heart, such as trenbolone; thus, the statement that oral steroids are worse than injectable steroids isn’t strictly true and is only partially accurate.
Can anabolic steroids be used in a non-toxic way?
Yes, we and other physicians throughout the world agree that certain anabolic steroids can be used in a safe manner when administered in a controlled medical environment in therapeutic dosages.
This is why there are several FDA-approved steroids utilized in medicine, such as testosterone, Deca Durabolin, and Anavar.
However, other steroids used in bodybuilding have high levels of toxicity and are not FDA-approved.
Bodybuilders obtaining anabolic steroids for cosmetic purposes and utilizing them without the supervision of a doctor is, in our experience, an unsafe practice.
Furthermore, when a patient is prescribed an FDA-approved steroid, it is guaranteed to be the real compound, being synthesized by a certified pharmaceutical company. However, bodybuilders buying steroids through the black market carry their own risks and dangers due to illegalities and a lack of regulations.
How fast do steroids work?
Some anabolic steroids work very fast. We have found testosterone undecanoate to peak serum testosterone levels within 5 hours of the first dose.
Fast-acting steroids are made up of short esters and do not need to be cycled for long durations in order to see significant results.
However, other steroids, such as Deca Durabolin, are made up of longer esters and are slower to have an effect.
Testosterone enanthate and cypionate are two more compounds that have longer half-lives and thus need to be cycled for at least 8 weeks, enabling enough time for them to kick in and for users to see maximum results.
Do steroids make you angry?
Anabolic steroids can make users increasingly angry and cause roid rage in certain individuals.
This is due to significantly higher testosterone levels, the male hormone that is responsible for increased levels of aggression.
However, steroids affect people in different ways, and some users do not experience increased outbursts of anger but instead more regular cases of irritation and grumpiness. We have not found roid rage to be a concern for most of our patients.
Do steroids show up on a drug test?
Anabolic steroids are banned substances by sporting federations such as WADA; thus, they will almost certainly show up on a drug test unless measures are put in place to mask their presence.
Army and police drug tests are generally designed to detect marijuana, cocaine, amphetamines, and opiates (not steroid metabolites). This is due to anabolic steroid tests being costly.
However, steroid tests may be specifically ordered if someone in the army or police force is to regularly talk about their steroid use. However, if a person is discreet, this is unlikely to be a problem, with some police officers showing obvious signs of steroid use.

Do steroids cause hair loss?
Yes, we have seen anabolic steroids cause hair loss due to significantly higher testosterone levels converting to DHT (dihydrotestosterone) via the 5α-reductase enzyme.
DHT can damage hair follicles due to its inflammatory effects on the scalp, causing miniaturization or loss of hair.
We find androgenic steroids to be the worst for accelerating hair loss due to them being DHT derivatives or having high levels of the 5α-reductase enzyme present.
A few examples of such compounds are:
- Anadrol
- Testosterone
- Trenbolone
However, androgenic alopecia (hair loss) is often genetic, and thus some users may experience hair loss that they are already predisposed to.
We have seen numerous steroid users with thick hair due to strong genetics in regard to follicle health and reduced natural levels of 5 AR.
Weak androgenic steroids can also be utilized to reduce or prevent hair loss during a cycle, such as Dianabol, Deca Durabolin, or Primobolan. These were compounds regularly used throughout the Golden Era, when many classic bodybuilders had thick hair.
Note: We have found it common for users to notice hair thinning or loss reverse post-cycle as DHT levels drop back into a normal range. However, such a reversal may not take place if ample time isn’t taken off in between AAS cycles to reduce inflammation on the scalp.
Can steroids make you infertile?
Yes. Based on our anecdotal findings and existing medical research, anabolic steroids have a direct damaging effect on the testicles (4), decreasing sperm count and quality.
This is an evolutionary irony known as the Mossman-Pacey paradox, where men take steroids to increase their sexual attractiveness but end up lowering their fertility (5).
Anabolic steroids cause the pituitary gland to cease producing LH and FSH (6) due to excessive testosterone levels. These two endogenous hormones are crucial in the production and health of sperm (7); thus, a deficiency can result in men becoming sterile.
Professor Alan Pacey believes 90% of steroid users could become sterile. Such a belief correlates with our findings.
Co Authors :

Dr. Thomas O’Connor is the first American board-certified internist to focus his medical practice specifically on the health and recovery of individuals who use anabolic steroids and androgens.
He founded Testosteronology®, a dedicated subspecialty of internal medicine that addresses steroid-induced hypogonadism and associated cardiovascular and metabolic concerns.
Dr. O’Connor has over 20 years of experience treating men and women with a history of anabolic steroid, SARM, and PED use. He has been a board-certified MD since 2005 and provides guidance on harm reduction methodologies.
Dr. O’Connor is a clinical instructor at the University of Connecticut School of Medicine and has been featured in various media publications, including Generation Iron, Dr. Phil, National Geographic, The New York Times, Muscle and Fitness, and others.
Dr. O’Connor also co-authored the largest survey on anabolic steroid use, which involved 2,385 men and was published in the peer-reviewed American Journal of Men’s Health. He holds active medical licenses in Connecticut and Florida.
References
(1) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3892473/
(2) https://www.sciencedaily.com/releases/2016/09/160913184951.htm
(3) https://pubmed.ncbi.nlm.nih.gov/28500659/
(4) https://bjui-journals.onlinelibrary.wiley.com/doi/10.1111/j.1464-410X.2011.10131.x
(5) https://onlinelibrary.wiley.com/doi/10.1111/joim.12885
