Top 5 Dianabol Stacks for Enhanced Muscle Growth
 Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
Disclaimer: The following article is for educational purposes only and does not promote or endorse the use of illegal steroids. For any questions or concerns, Dr. Touliatos is available for consultation.
Dianabol, or methandrostenolone, is the leading oral anabolic steroid available. We have observed novices experience weight increases of up to 30 pounds from a Dianabol-only cycle.
Nevertheless, after numerous solo cycles, users will start to plateau.
For those seeking to increase strength and muscle hypertrophy further, a Dianabol stack is an effective methodology for achieving such.
Stacking Dianabol entails the simultaneous administration of an additional steroid or multiple steroids. Since Dianabol primarily functions as a bulking steroid, people typically stack it with other mass-building compounds during the off-season. Typically, these compounds are:
- Anadrol
- Testosterone
- Deca Durabolin
Contents
We will examine the most prevalent Dianabol stacks used by bodybuilders from the Golden Era to the present day. We will provide cycle information on the appropriate dosages and durations of use.
Top 5 Dianabol Stacks
Dianabol and Nandrolone Stack
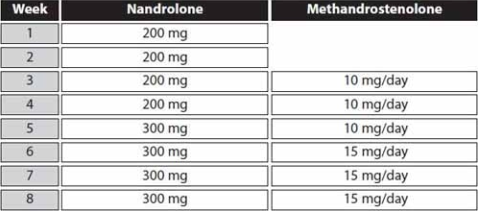
The aforementioned cycle represents mild dosages. However, more experienced steroid users may prefer to increase the Dianabol dose to 20 mg/day and the Deca Durabolin dose to 500 mg/week.
A Dianabol and Deca Durabolin stack is a common bulking protocol, with numerous bodybuilders from Arnold Schwarzenegger’s era utilizing this stack during the off-season to accumulate as much mass as possible.
Dianabol is an oral steroid, while Deca Durabolin is an injectable. Consequently, the inclusion of Deca Durabolin does not cause any additional liver strain, which is crucial given the hepatotoxic nature of Dianabol.
Only users who have cycled Dianabol and tolerated it should take this stack. Deca Durabolin will enhance strength and size gains while simultaneously suppressing testosterone levels and contributing to further water retention.
This stack is effective in reducing hair loss during a cycle, as far as steroids are concerned. We can attribute this to the fact that neither compound is particularly androgenic. Consequently, dihydrotestosterone (DHT) levels will not rise significantly.
Adverse Effects:
- Impotence
- Hepatotoxicity
- Hypogonadism
- Edema
- Gynecomastia
Supplements
Our patients typically consume the following supplements to minimize side effects from a Dianabol and Deca Durabolin stack:
- Fish oil: 4 g/day
- TUDCA: 500 mg/day
- Letrozole: 1.25 mg every other day
- Dostinex: 0.5–1 mg per week
Our patients have successfully reduced cardiotoxicity, hepatotoxicity, progesterone, and estrogen with the above supplements. Users should take these supplements throughout the entire cycle.
Fish oil will assist in the regulation of blood pressure, which will undoubtedly increase as a result of this stack, with Dianabol being the primary culprit. This cardiac strain can be attributed to Dianabol being an oral steroid. We have observed numerous oral steroids activate hepatic lipase during their passage through the liver. Regrettably, this enzyme substantially reduces high-density lipoprotein (HDL), which is the cardioprotective form of cholesterol (1).
Furthermore, increased water retention from Dianabol use has a detrimental impact on blood pressure, necessitating the heart to exert more effort than usual to circulate blood throughout the body. Additional blood viscosity, caused by greater volumes of H₂O, is the cause of this.
Tauroursodeoxycholic acid (TUDCA) is a naturally occurring substance in bile that aids restoration of the liver. The supplement form provides steroid users with higher quantities of this natural, liver-protecting substance (2).
We have found Dianabol to be among the most deleterious steroids concerning hepatic health. TUDCA supplementation is therefore imperative.
Gynecomastia is a potential consequence of the use of Dianabol and Deca Durabolin. Dianabol’s high aromatizing properties can induce the development of breast tissue in males.
According to our data, the most efficient method for preventing gynecomastia is to take either an aromatase inhibitor (AI) or a selective estrogen receptor modulator (SERM). In general, SERMs are more advantageous than AIs since they do not exacerbate cholesterol levels and blood pressure (3).
However, Nolvadex and Clomid can worsen progesterone-related side effects. As a consequence of an increase in progesterone, a hormone that is comparable to estrogen, Deca Durabolin has the potential to cause gynecomastia. Thus, we typically monitor patients’ nipples with this stack, and if they start to become swollen or breast tissue enlarges, then we administer an AI to prevent further hypertrophy.
Letrozole is an effective AI that reduces the conversion of testosterone into estrogen (4), which is effective for combating high progesterone. We have found SERMs to be ineffective in reducing progesterone-induced gynecomastia from Deca Durabolin.
We frequently observe Deca Durabolin eliciting impotence during a cycle, which can have an unfortunate effect on the sexual health of male users. This is the result of Deca Durabolin’s significantly increasing prolactin levels. We prescribe cabergoline to patients to address this imbalance, inhibiting the production of prolactin and maintaining libido.
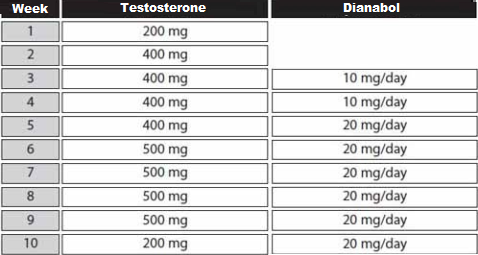
Dianabol and Testosterone Stack
Dr. John Ziegler was entrusted with developing a steroid that was more potent than testosterone in order to assist the US Olympic team in defeating the Soviets in the 1950s. Thus, historically, Dianabol and testosterone were once archenemies.
Dr. Ziegler subsequently created methandrostenolone, more widely known as Dianabol. Dianabol had an anabolic rating that was higher than that of testosterone, and its androgenic effects were less pronounced.
Thus, Dianabol and testosterone function similarly; however, Dianabol is superior in the context of muscle development, whereas testosterone excels at fat reduction due to its higher androgenic properties.
The most significant distinction between the two is that Dianabol is an oral steroid, whereas testosterone is an injectable. This results in a complementary pairing, as users are essentially stacking another form of exogenous testosterone without additional liver toxicity.
This is one of the most successful Dianabol stacks we have observed in regard to gaining muscle without excessive toxicity.
Any testosterone ester may be utilized for this stack; however, the most popular forms are:
- Enanthate
- Cypionate
Adverse Effects
In terms of side effects, testosterone suppression will be more dramatic with this stack compared to a Dianabol-only cycle. Thus, diligent post-cycle therapy (PCT) is necessary to prevent testosterone deficiency syndrome (TDS).
Cholesterol levels will rise higher than when taking Dianabol alone. Nevertheless, we have found testosterone to be the most cardiovascular-friendly steroid. Thus, cholesterol levels will not experience dramatic elevations in comparison to a Dianabol-only cycle.
This stack considerably raises the risk of developing gynecomastia, as both steroids are estrogenic. Consequently, it is imperative to utilize a selective estrogen receptor modulator (SERM) such as Nolvadex during the cycle.
It is also probable that users will experience some androgenic adverse effects, such as benign prostatic hyperplasia, male pattern baldness, seborrhea, or acne vulgaris.
Supplements
- Fish oil: 4 g/day
- TUDCA: 500 mg/day
- Nolvadex: 30 mg/day
We advise users to take these supplements for the entire cycle.
Dianabol and Trenbolone Stack
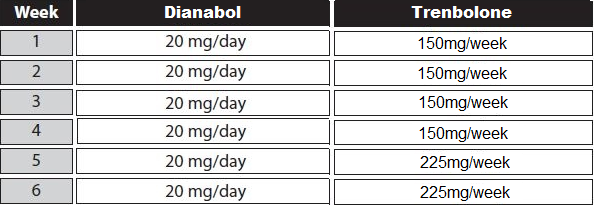
The high toxicity of this stack dictates that it be employed exclusively by advanced steroid users. Consequently, these dosages are regarded as moderate to high and are designed for a seasoned user.
Dianabol and trenbolone should be perceived as a more potent and severe stack than Dianabol and testosterone.
Trenbolone, like testosterone, is an injectable medication. Trenbolone operates in a manner that is significantly distinct from Dianabol, as it does not aromatize or induce water retention. Consequently, we observe less overall weight gain when using trenbolone. Despite this, trenbolone’s capacity to augment the physique with lean muscle tissue is comparable to that of Dianabol.
Trenbolone is extremely androgenic, with a rating of 500, roughly 10 times that of Dianabol.
Therefore, trenbolone can cause notable fat loss as it increases the stimulation of androgen receptors (AR), inducing lipolysis. This is in conjunction with adding exceptional amounts of lean muscle.
Some might question the rationale behind stacking trenbolone with Dianabol, given that the former does not induce aromatization and the latter has an opposing effect. Despite such a notion, users can administer this stack in the offseason to achieve remarkable results in hypertrophy.
In contrast, incorporating a Dianabol and trenbolone stack during the summer may be unfavorable, as Dianabol can counteract the diuretic effects of trenbolone. This can compromise muscle definition.
Users frequently experience noteworthy muscle growth as a result of this stack, regardless of its timing.
Adverse Effects
Liver toxicity will be notable solely due to Dianabol; trenbolone will not enhance hepatic strain.
Gynecomastia is a significant risk associated with this stack, as Dianabol elevates estrogen and trenbolone heightens progesterone. When combined with an aromatizing steroid, such as Dianabol, we observe more incidents of progesterone-induced gynecomastia.
Aromatase inhibitors (AIs) are the most effective option for preventing gynecomastia while administering this stack, based on our experience. Conversely, AIs will spike blood pressure levels, which is not desirable. Therefore, this stack is unsuitable for individuals who are at risk of cardiomyopathy or have concerns regarding gynecomastia.
Androgenetic alopecia, seborrhea, and acne vulgaris are possible with this stack due to trenbolone’s high androgenicity.
These are generally transient side effects, with bouts of acne and hair loss commonly resolving post-cycle. Even so, the use of androgenic steroids for an extended period of time may result in more severe and enduring adverse effects.
Our patients can experience significant testosterone suppression from this stack. It is feasible that users’ natural testosterone levels will require several weeks or months to recover, even with an effective PCT.
Supplements
- Fish oil: 4 g/day
- TUDCA: 500 mg/day
- Letrozole is optional. Users can take 1.25 mg every other day to control estrogen if blood pressure is within a normal range.
Dianabol and Oxymetholone Stack
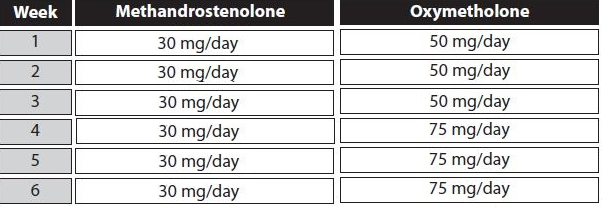
Anadrol is the more popular name for oxymetholone. This particular cycle is strongly dosed; thus, it is presumed that only experienced steroid users will utilize this stack, as they are more adept at sustaining larger doses. Beginners should refrain from following this protocol, and intermediates may administer smaller doses than listed in this cycle, with Dianabol dosed at 20 mg and Anadrol at 50 mg.
The most efficient stack for achieving maximum mass and weight gain is to combine Dianabol and Anadrol.
The toxicity of this stack rivals that of Dianabol and trenbolone.
The compounds Dianabol and Anadrol are highly estrogenic oral steroids that are both extremely efficacious in building muscle and strength.
Both anabolic steroids will cause significant fluid retention. Yet their chemical structures are somewhat distinctive, with Dianabol being a derivative of testosterone and Anadrol being a derivative of dihydrotestosterone.
Dianabol also increases estrogen levels by means of aromatase, whereas Anadrol does not aromatize but directly stimulates estrogen at a receptor level.
Adverse Effects
We find liver toxicity to be a significant issue with this stack, as Dianabol and Anadrol are both hepatotoxic oral substances. Individuals with liver conditions should refrain from applying this stack.
We also recommend keeping cycles relatively brief to minimize harm to this organ. A person can usually reverse liver damage and inflammation from this stack if they cease drinking alcohol, refrain from taking other hepatotoxic drugs, and supplement with milk thistle and TUDCA.
The liver is a highly resilient organ that is capable of withstanding years of maltreatment before succumbing to its condition. Therefore, during the intervals between cycles, the liver typically recovers, and the elevated enzymes return to their normal levels.
A Dianabol and Anadrol stack is the most deleterious for users’ liver and heart health. Significant shifts in LDL and HDL cholesterol levels can be experienced from this duo, resulting in exceedingly high blood pressure readings over 180/120 mmHg.
It is imperative to consume fish oil and engage in regular cardiovascular exercise to prevent hypertension.
From the starting point of this cycle, it is imperative that users are in excellent cardiovascular health. Users should also undergo routine bloodwork during the cycle to promptly detect any complications.
We strongly discourage the use of AI inhibitors, as they can worsen cardiac health. Furthermore, an AI does not prevent gynecomastia on Anadrol. However, our patients have administered SERMs with such stacks, including Nolvadex, enabling us to control and avoid breast tissue formation.
Anadrol is a DHT derivative and thus very androgenic. Consequently, we have observed cases of acne vulgaris and balding in individuals genetically prone to these conditions.
Endogenous testosterone production will shut down post-cycle on Dianabol and Anadrol, with the pituitary gland signaling to the testes to halt production. Thus, an aggressive PCT will mitigate the unavoidable decline that occurs post-cycle.
Supplements
- Fish oil: 4 g/day
- TUDCA: 500 mg/day
- Nolvadex: 30 mg/day
These supplements are to be taken for the whole duration of the cycle.
Many find this to be a peculiar stack, as Anavar is often described as a cutting steroid and Dianabol a bulking steroid. Even so, it is remarkable that a significant number of individuals are interested in stacking such a duo together. Anavar is utilized to enhance strength, reduce fat mass, and add small to moderate amounts of muscle mass.
A person may stack Dianabol and Anavar in tandem if they are uncomfortable with injections.
Generally, we find that combining oral anabolic steroids together produces harsh side effects. However, in this case, the stack is relatively mild due to the minimal risk associated with Anavar. Additionally, blood pressure levels will not be significantly elevated in comparison to a Dianabol-only protocol. We have observed that Anavar is extremely prevalent among both sexes, as both men and women have experienced no side effects.
Stacking Dianabol with Anavar will increase lean muscle mass while reducing subcutaneous fat mass. Thus, users may utilize this stack to gain lean muscle mass. This could, therefore, be classified as a bulking cycle.
Nevertheless, if users are concerned about muscle loss and are in the process of cutting, combining Dianabol with Anavar will significantly reduce catabolism, as opposed to taking Anavar in isolation. Therefore, certain bodybuilders may be amenable to gaining a small amount of water in exchange for preserving their muscle size.
Dianabol, as we are aware, induces substantial water retention. Conversely, Anavar has the opposite effect, expelling extracellular fluid from the body.
Consequently, the inclusion of Anavar can alleviate water retention and edema associated with Dianabol. However, because Anavar positively redistributes water levels within the muscle cells, we often observe muscle fullness increasing further.
Adverse Effects
Although Anavar is one of the safest steroids in our experience, it is not free from adverse effects.
Testosterone suppression will be heightened as opposed to taking Dianabol alone. Users may also experience extra hair thinning on their scalp, as well as some extra liver strain.
Anavar is also very expensive, so if you’re looking for a cheap Dianabol stack, this may not be for you.
Supplements
- Fish oil: 4 g/day
- TUDCA: 500 mg/day
- Nolvadex: 30 mg/day
Frequently Asked Questions
What Should I Use for a PCT?
PCT is recommended for all the above stacks to regulate hormone production, particularly testosterone.
The three main PCTs we utilize are:
- HCG: 2000 IU administered every other day for 20 days
- Tamoxifen (Nolvadex): 2 x 20 mg for 45 days
- Clomiphene (Clomid): 2 x 50 mg for 30 days
If you have taken Nolvadex during a cycle, it would be more optimal to use Clomid and HCG for the PCT.
As testosterone suppression is likely to be significant in many of the above stacks, we recommend combining all of the PCT medications simultaneously, or, at a minimum, running HCG and Clomid together. This will be more effective than merely using one of these medications.
Bodybuilders often buy the above PCT drugs from the black market instead of having them prescribed by a doctor. This way, they can take them wherever they want in the right dosages, rather than being limited by prescription dates or the doctor’s command.
Muscle Retention Post-Cycle
In terms of weight gain, we find users will lose some water post-cycle, and thus the number on the scale may decrease. This is especially true when Dianabol is stacked with other wet compounds, such as:
- Anadrol
- Testosterone
However, in relation to lean muscle gains, if the person continues to train hard after their cycle and runs a sufficient PCT, they should be able to retain virtually all of their gains.
Summary
The two best Dianabol stacks in our experience are:
- Dianabol and Deca Durabolin
- Dianabol and testosterone
This is because Deca Durabolin and testosterone complement Dianabol’s powerful mass-building effects in the off-season without causing overly harsh side effects.
Despite the exceptional gains that Anadrol and trenbolone produce, we have seen them cause devastating effects on overall health, especially to the heart and liver.
Anavar and Dianabol simply do not complement each other; however, they may be an effective combination for a specific person in the correct situation. I.e., if someone is anxious about losing muscle or strength when cutting.
Co Authors :

Dr. Thomas O’Connor is the first American board-certified internist to focus his medical practice specifically on the health and recovery of individuals who use anabolic steroids and androgens.
He founded Testosteronology®, a dedicated subspecialty of internal medicine that addresses steroid-induced hypogonadism and associated cardiovascular and metabolic concerns.
Dr. O’Connor has over 20 years of experience treating men and women with a history of anabolic steroid, SARM, and PED use. He has been a board-certified MD since 2005 and provides guidance on harm reduction methodologies.
Dr. O’Connor is a clinical instructor at the University of Connecticut School of Medicine and has been featured in various media publications, including Generation Iron, Dr. Phil, National Geographic, The New York Times, Muscle and Fitness, and others.
Dr. O’Connor also co-authored the largest survey on anabolic steroid use, which involved 2,385 men and was published in the peer-reviewed American Journal of Men’s Health. He holds active medical licenses in Connecticut and Florida.
References
(1) https://pubmed.ncbi.nlm.nih.gov/7076794/
(2) https://pubmed.ncbi.nlm.nih.gov/31236688/
(3) https://pubmed.ncbi.nlm.nih.gov/16109320/
(4) https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2001216/
